Arcot J Chandrasekhar, M.D.
 |
Adhesive Atelectasis / ARDS
Diffuse bilateral lung atelectasis due to ARDS. There is loss of surfactant with resultant atelectasis of alveoli.
There is diffuse white out of lungs.
The lungs are small. |
|

|
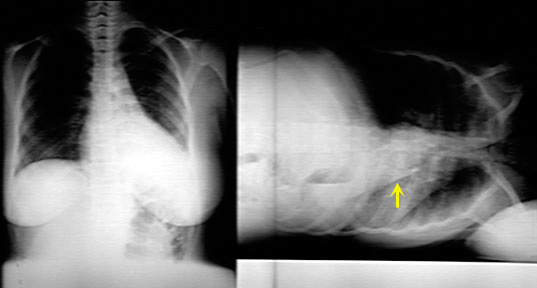
Plate like atelectasis
Plate like atelectasis (sub segmental atelectasis) is an example of focal loss of surfactant.
Note the bilateral basal plate like atelectasis.
This is an example of plate like atelectasis (yellow arrows) in a patient with pulmonary embolism.
You can also encounter plate like atelectasis whenever there is basal hypo ventilation.
|
|
|
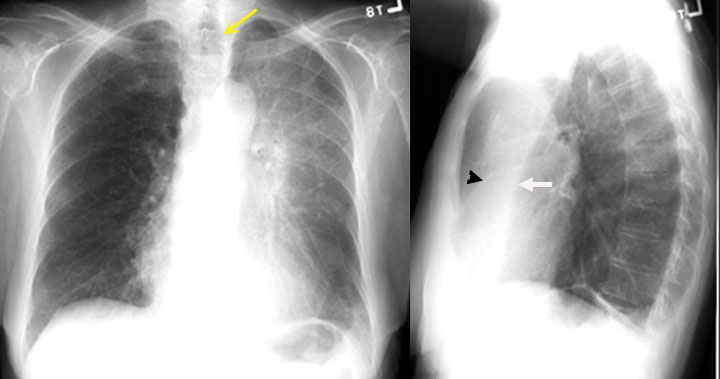
RUL atelectasis
- Density in projection of the right upper lung field.
- Triangular in shape with narrow end towards the hilum (lobar configuration).
- Transverse fissure has moved up (white arrow).
- Right hilum has moved up.
- In the lateral view, the transverse fissure has moved up towards the oblique fissure (Black arrow).
- All signs of RUL lung volume loss.
This is resorptive atelectasis due to bronchial obstruction (cancer
lung).
|
|

|
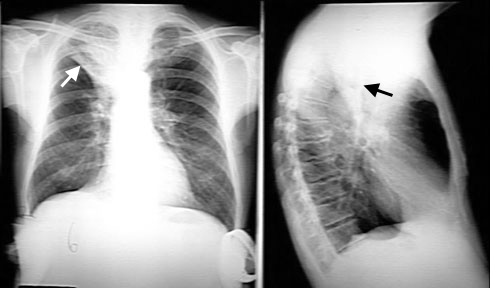
RLL Atelectasis
The adjacent CXR shows density in the projection of the right lower lung field. The right heart border is seen clearly while the diaphragm is indistinct, indicating that it is lower lobe disease (silhouette sign).
The shadow is triangular with narrow end near the hilum, suggesting that it is lobar density.
The right hilum and transverse fissure are pulled down (loss of lung volume). Arrows are pointing to the hila position on both sides.
In complete RLL atelectasis you will not see the right inter lobar artery because it is surrounded by airless lung (silhouette sign).
This is an example of right lower lobe resorptive atelectasis. Bronchial obstruction is due to endobronchial lung cancer.
|
|
|
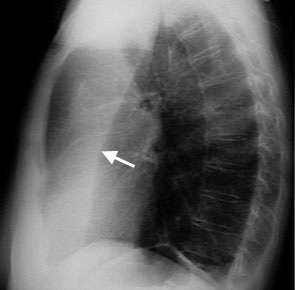
RML atelectasis
Vague density in the right lower lung field. It can easily be missed in PA view.
Minor loss of right heart silhouette.
Triangular density in the lateral chest with narrow end towards hilum.
Loss of lung volume:
- Movement of transverse fissure (White arrow) towards the oblique fissure.
- Volume of RML is less than 5% of total lung volume and as such you will not see elevation of right hilum in PA view chest.
This is a case of RML resorptive atelectasis due to obstruction of the RML. |
 |
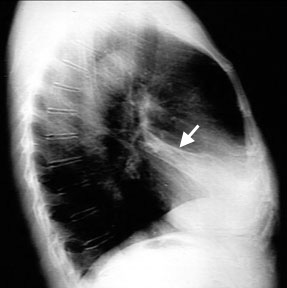
LUL Atelectasis
Haziness in the projection of the left upper lung field in PA view. Band of increased density in the retrosternal space in lateral chest (airless lung).
Loss of left heart silhouette indicating that the lingula is abnormal.
Loss of lung volume:
Note the compensatory hyper inflation of left lower lobe behind the oblique fissure in the lateral chest. See the lower lobe creep up all the way up to the apical region (luft sichel sign)
This is a case of resorptive atelectasis due to endobronchial obstruction of the LUL. |
 |
LLL Atelectasis
Atelectatic LL moves to retro cardiac location and projects as a triangular density (yellow arrow) seen through heart. Lateral decubitus film shows clearly the triangular atelectatic left lower lobe behind the heart.
Left hilum moves down (sign of loss of lung volume).
In the lateral chest (not shown), atelectatic LL projects over lower thoracic vertebra. Instead of uniform density of thoracic vertebra from top to bottom you will see lower thoracic vertebra appear denser than upper thoracic vertebra.
As with other lobar atelectasis you will not see the lower lobe vessels. The medial portion of left diaphragm will become indistinct (silhouette sign).
|
 |
Total atelectasis of Lung
The right hemi thorax is whited out (no air). Signs of loss of lung volume include:
- Trachea is shifted to the right (yellow arrow)
- Hemi thorax is smaller on the right
- Crowding of ribs on the right
Silhouette sign:
The silhouette of the right heart and right hemi diaphragm are lost.
Vessels in right lung not seen due to loss of air in alveoli
|
When you are considering resorptive
atelectasis make the following statements to support it.
- Triangular density.
- Signs of loss of lung volume. Indicate the evidence
- Localize it to a segment, lobe or lung. (Use silhouette sign)
- Compensatory hyperinflation.
- Etiology: Look for what is causing endobronchial obstruction
(coin, mass, mal position of ET tube etc)
Most of the time you will not see anything obvious to account for
obstruction. You have to suspect the etiology of obstruction based on the
history and the clinical setting.
- Post op: Mucus plug
- Heavy smoker: Lung cancer
- Healthy child eating peanuts: Aspiration
- On ventilator with ET tube in right main stem bronchus
|
|
When you are considering relaxation atelectasis make the following
statements to support it.
- The primary event is in the pleural space, like
pneumothorax.
- Trachea will be shifted to opposite side because of
the primary pleural event.
- The entire lung will be atelectatic.
- Etiology is usually pneumothorax. (You will not see
the atelectatic lung underneath the effusion. Silhouette sign)
|
|
When you are considering adhesive atelectasis make the following
statements to support it. This occurs when there is no surfactant.
Diffuse:
-
Diffuse white out with smaller lungs
-
Etiology: ARDS or Neonatal RDS (hyaline membrane
disease)
When it is plate like atelectasis it is either due
to loss of CO2 or oxygen. CO2 and oxygen maintain the integrity of
surfactant.
-
Basal hypo ventilation
-
Lack of Oxygen (pulmonary embolism)
Basal hypo ventilation can be seen in
-
Post op state
-
Obesity
-
Acute abdomen
-
Diaphragmatic paralysis
Look at the clinical setting to determine the etiology of
adhesive atelectasis.
|