Consolidation
Arcot J Chandrasekhar, M.D
Objectives:
- Relate pathology of consolidation to image findings
- Radiological criteria to call a density as consolidation
- Example of consolidation of various lobes
 |
 |
|
One whole lobe is consolidated with decreased crepitation. The size of the affected lobe is normal. However, the color is dark red. The cut surface may ooze fluid, which may be hemorrhagic or purulent. Airways of the affected lobe may contain pus. This gross photograph of a cut lung shows consolidation and discoloration of most of the lower lobe. |
|
| Pathology | Imaging | Physical examination |
| Lobar involvement | Lobar density | Findings over surface representing lobe |
| Airspace filled with inflammatory exudates | Liquid density | Dullness to percussion |
| Patent bronchi | Air bronchogram | Bronchial breathing, bronchophony |
| No significant loss of lung volume | No signs of loss of lung volume | No signs of loss of lung volume |
| Pleural inflammation | Blunting of costophrenic angle | Pleural rub |
| Stage of resolution | Crackles | |
| Decreased chest expansion on affected side |
Radiological criteria
Lobar / Segmental density
-
The lobe is made up of in excess of 99% alveoli. Hence, if you see a lobar density with no loss of lung volume, the disease is primarily in the alveoli. It is a homogenous radio opaque density obscuring vessels.
-
Lobar and segmental densities are triangular, narrow towards the hilum and broad towards the chest wall.
-
Consolidation will not cross a fissure.
Air bronchogram
- Bronchi are visible only up to the fourth order of branching. You can see the trachea, main stem bronchi and the next order of bronchi. Elastic cartilage decreases with each order of branching. Distal bronchi are surrounded by air filled alveoli. There is no contrast between air filled bronchi and surrounding air filled alveoli. Thus, the bronchi are not visible. If the alveoli are filled with liquid density (pneumonia, edema, and hemorrhage, etc.) there is contrast with air filled bronchi and they become visible as branching tubular structures through the density.
- Thus, the visible air bronchogram implies that there is alveolar filling and the bronchi are patent.
No significant loss of lung volume
-
When the alveoli are filled with either inflammatory exudates, hemorrhage or edema they retain their size and do not show signs of lung volume loss. In the early stages of pneumonia, lung volume increases slightly. In Klebsiella pneumonia where the inflammatory exudates is heavy, the volume of the lobe can actually increase giving the radiological sign "bulging fissure sign". When alveoli are empty, with loss of air, it is called atelectasis.

RUL Consolidation
- Lobar density: There is opacity in the projection of the right upper lung field corresponding to RUL. It is a triangular density.
- Consolidation extends to pleura and transverse fissure. Note that consolidation does not cross transverse fissure.
- Air bronchogram: You can see the air filled bronchi coursing through the density.
- The trachea is in midline and the transverse fissure is in its normal location (slightly retracted upwards), indicating that there is no significant loss of lung volume.

RML Consolidation
-
Radio opaque density in the projection of right lower lung field.
-
The right diaphragm is clearly seen, excluding lower lobe disease.
-
The right heart margin is indistinct, indicating right middle lobe disease (silhouette sign).
-
In the lateral chest x-ray you see a triangular density narrow at hilum and broad towards the chest wall corresponding to RML.
-
The transverse fissure and oblique fissures are in their normal location. No loss of RML lung volume.
-
There is air bronchogram, but it is not seen clearly in this presentation.

LUL Consolidation
-
The left heart border is obliterated with most of the left upper lung white with black branching density.
-
There is loss of aortic and left heart silhouette, indicating LUL disease (silhouette sign). Left hemi diaphragm is clearly seen indicating normal lower lobe.
-
Branching black tubular density is the air bronchogram.
-
In the lateral view, the oblique fissure is in its normal location with density anterior to it corresponding to LUL (no loss of lung volume).


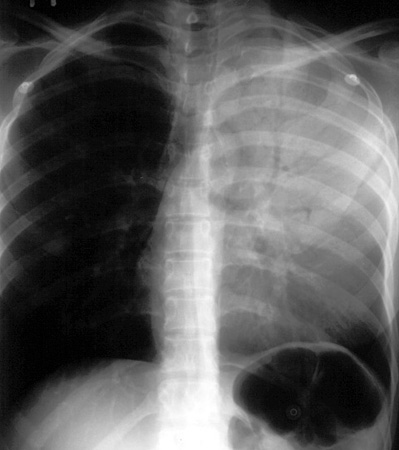
Lingular consolidation
It looks like RML consolidation, but on the left side.
-
Density in the projection of the left lower lung field.
-
The left heart border is fuzzy, suggesting lingular disease (silhouette sign).
-
The left diaphragm is seen clearly, excluding LLL disease.
-
The left costophrenic angle is obliterated, suggesting small left pleural effusion.
-
In the lateral chest view a triangular density with narrow end towards the hilum and the broad surface towards the chest wall corresponding to lingula.
-
The left oblique fissure and accessory transverse fissure are normal in location, indicating no loss of lung volume.